

Are you a new member? Sign up now
Login area
| Sign up
Let us help you
Read about the latest topics.
Read about the latest topics.


Universal Health Coverage: Bridging the Gaps
Universal Health Coverage:
Bridging the Gaps [1]
Walid Ammar MD., Ph.D.[2]
Bridging the Gaps [1]
Walid Ammar MD., Ph.D.[2]
- Universal Health Coverage and the Lebanese Dilemma
Achieving Universal Health Coverage (UHC) is a main goal of the National Health Strategy, and is based on the principles of justice, equity, poverty reduction and the rational use of resources. It requires financing or providing preventive and curative quality health care for all, to satisfy each one’s needs against affordable contributions. Whereas alleviating the financial burden, as much as possible, on households, especially the poor, remains a main objective of UHC.
The purpose of Universal Health coverage is to ensure universal accessibility to services that address population health needs and country health priorities with adequate quality, without incurring households financial ruin. This implies reaching a consensus over two major policy decisions: 1st defining a benefit package, and 2nd, setting an acceptable level of financial burden on households, more specifically the OOP bearable level by income category. Starting up from scratch, the benefit package would include essential health services such as PHC, and the government would cover as much health interventions as its budget allows, by beginning with the most cost effective ones such as immunization, TB treatment and prenatal care. Thus the population would expect regular upgrading of the system and would welcome incorporating progressively more advanced services such as renal dialysis, treatment for cancer, and sophisticated surgeries. The dilemma of the health system in Lebanon is the current existence of a universal coverage for tertiary care and sophisticated treatments such as open heart and joint replacement surgeries and expensive cancer patent drugs, whereas, paradoxically, prevention and PHC services are not universally covered.
The purpose of Universal Health coverage is to ensure universal accessibility to services that address population health needs and country health priorities with adequate quality, without incurring households financial ruin. This implies reaching a consensus over two major policy decisions: 1st defining a benefit package, and 2nd, setting an acceptable level of financial burden on households, more specifically the OOP bearable level by income category. Starting up from scratch, the benefit package would include essential health services such as PHC, and the government would cover as much health interventions as its budget allows, by beginning with the most cost effective ones such as immunization, TB treatment and prenatal care. Thus the population would expect regular upgrading of the system and would welcome incorporating progressively more advanced services such as renal dialysis, treatment for cancer, and sophisticated surgeries. The dilemma of the health system in Lebanon is the current existence of a universal coverage for tertiary care and sophisticated treatments such as open heart and joint replacement surgeries and expensive cancer patent drugs, whereas, paradoxically, prevention and PHC services are not universally covered.
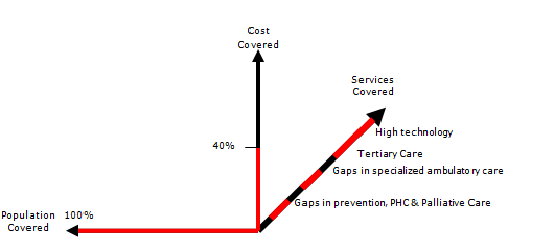
Therefore, while the population is looking up for more and more technologically advanced interventions, the public opinion would not be particularly enthusiastic about enhancing the coverage of essential services such as introducing new vaccines to the immunization calendar, mental health and safe motherhood care. Consequently, politicians would not venture a UHC plan that may disappoint their voters.
Nevertheless, technically, the main issue for achieving UHC in Lebanon remains the accessibility to a comprehensive package of PHC services including promotive, preventive and palliative care in addition to early diagnosis and early treatment.
- Scaling-up PHC and reducing OOP as a Strategic Direction
The 1998 National Health Accounts revealed that Total Health Expenditures (THE) represented 12.3% of GDP of which 60% were Out-Of-Pocket (OOP) payments. There is no doubt that oversupply in addition to focusing on financing curative care, and the poor quality of preventive and primary health care at that time, have contributed to over consumption of expensive diagnostics and treatments provided by the private for profit sector.
The MOPH historically covers In-patient services and expensive treatments. Ambulatory services were mostly uncovered, and therefore most OOP were spent on medication and outpatient services. The development of a wide network of PHC centers providing quality services that are accepted as an alternative for the private outpatient care, became the main goal of the MOPH to ensure universal accessibility to health care.
The success of the MOPH in decreasing the THE to 7.5% of the GDP in 2012 mainly by decreasing the OOP to reach 37% of THE, confirms the pertinence of reorienting its strategy towards PHC, especially that rationalization of households health expenditure was associated with an increased utilization of health services along with quality improvement. This was consolidated by a positive overall impact documented by a significant improvement in health indicators. Nevertheless, the OOP is still considered relatively high which requires moving further along the same strategic direction towards achieving UHC.
The MOPH historically covers In-patient services and expensive treatments. Ambulatory services were mostly uncovered, and therefore most OOP were spent on medication and outpatient services. The development of a wide network of PHC centers providing quality services that are accepted as an alternative for the private outpatient care, became the main goal of the MOPH to ensure universal accessibility to health care.
The success of the MOPH in decreasing the THE to 7.5% of the GDP in 2012 mainly by decreasing the OOP to reach 37% of THE, confirms the pertinence of reorienting its strategy towards PHC, especially that rationalization of households health expenditure was associated with an increased utilization of health services along with quality improvement. This was consolidated by a positive overall impact documented by a significant improvement in health indicators. Nevertheless, the OOP is still considered relatively high which requires moving further along the same strategic direction towards achieving UHC.
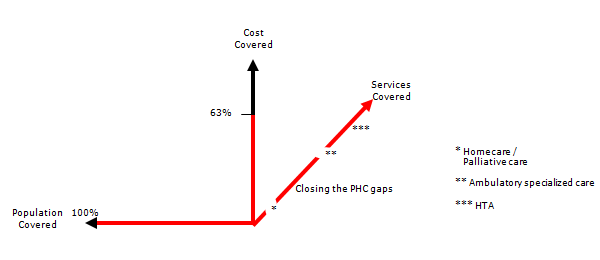
In addition a model for covering ambulatory specialized care in the public hospitals’ out-patient departments to fill this important gap in the current system, represent an affordable option assuming good adherence to the set rules, particularly the respect of the referral system by considering the PHC center as a gate keeper.
The cost born by the government for providing PHC and public secondary health services is equivalent to almost the third of the cost incurred by the individuals when purchasing themselves the services directly from the private sector.
In addition to the alleviation of the household financial burden by increasing government investment, part of direct disbursement upon utilization (OOP) could be shifted to a prepayment mode, through a community health insurance model. A World Bank financed project, designed to pilot this model by recruiting the extreme poor in a community “fidelity” scheme, is currently under implementation.
The cost born by the government for providing PHC and public secondary health services is equivalent to almost the third of the cost incurred by the individuals when purchasing themselves the services directly from the private sector.
In addition to the alleviation of the household financial burden by increasing government investment, part of direct disbursement upon utilization (OOP) could be shifted to a prepayment mode, through a community health insurance model. A World Bank financed project, designed to pilot this model by recruiting the extreme poor in a community “fidelity” scheme, is currently under implementation.
- The Cost of ensuring financial fairness through Universal Health Coverage
Calculating the cost of exempting the poorest and decreasing the contribution of the less poor, necessitates defining those categories and calculating their health spending. The current distribution of THE by source of health financing is as follows:
43% of THE are Out-of-pocket spending
27% of THE are General Government Spending. These include the totality of the MOPH budget, 25% of the NSSF spending, and health care budget items of the remaining public funds.
28% of THE are prepayments that include private insurance premiums and NSSF employees and employers contributions.
According to the Household Living Conditions Survey of 2004-2005, the OOP spending is distributed by income categories as follows: 30% paid by households with a monthly income lower than 650 thousand LBP; 30% by households earning between 650 thousand and 1,200,000; and finally the income category of more than 1,200,000, contribute the remaining 40% of the total OOP spending on health. Knowing that a significant proportion of the latest category spending is on supplementary and luxury goods and services like food supplements, cosmetics and plastic surgeries.
The target for achieving equity in health financing and alleviating poverty would be set as to achieve complete exemption of the poorest from any payment, and decrease the health spending of the less poor by half.
Considering that Total Health Expenditures (THE) represent around 7.41% of GDP and OOP spending 43% of THE, then OOP amounts to 3.19% of GDP. This is distributed over the three aggregated categories of income respectively 0.957%, 0.957%, 1.276%. Accordingly, the amount that needs to be alleviated from the households burdens amounts to 1.4355% of GDP (0.957%+0.957%/2).
If we consider the 2009 GDP of 53,000 Billion LBP; the estimated reduction of OOP would be around 760 Billion LBP. However, this does not mean that the cost incurred by the government needs to be as mush. From our experience, the cost born by the government for providing PHC and public secondary health services is equivalent to almost the third of the cost incurred by the individuals when purchasing themselves the services directly from the private sector. Accordingly, the estimated cost of the project would be around 250 Billion LBP which corresponds to increasing by 24% of total government spending on health in 2009. This estimate assumes good adherence to the set rules, particularly the respect of the referral system between the PHC centers and governmental hospitals, and the prescription of generic drugs. This might be ambitious to achieve in short term, nevertheless, the cost of the first stage of the project concerning the universal accessibility to essential services is perfectly affordable under current circumstances as shown in section VI.
43% of THE are Out-of-pocket spending
27% of THE are General Government Spending. These include the totality of the MOPH budget, 25% of the NSSF spending, and health care budget items of the remaining public funds.
28% of THE are prepayments that include private insurance premiums and NSSF employees and employers contributions.
According to the Household Living Conditions Survey of 2004-2005, the OOP spending is distributed by income categories as follows: 30% paid by households with a monthly income lower than 650 thousand LBP; 30% by households earning between 650 thousand and 1,200,000; and finally the income category of more than 1,200,000, contribute the remaining 40% of the total OOP spending on health. Knowing that a significant proportion of the latest category spending is on supplementary and luxury goods and services like food supplements, cosmetics and plastic surgeries.
The target for achieving equity in health financing and alleviating poverty would be set as to achieve complete exemption of the poorest from any payment, and decrease the health spending of the less poor by half.
Considering that Total Health Expenditures (THE) represent around 7.41% of GDP and OOP spending 43% of THE, then OOP amounts to 3.19% of GDP. This is distributed over the three aggregated categories of income respectively 0.957%, 0.957%, 1.276%. Accordingly, the amount that needs to be alleviated from the households burdens amounts to 1.4355% of GDP (0.957%+0.957%/2).
If we consider the 2009 GDP of 53,000 Billion LBP; the estimated reduction of OOP would be around 760 Billion LBP. However, this does not mean that the cost incurred by the government needs to be as mush. From our experience, the cost born by the government for providing PHC and public secondary health services is equivalent to almost the third of the cost incurred by the individuals when purchasing themselves the services directly from the private sector. Accordingly, the estimated cost of the project would be around 250 Billion LBP which corresponds to increasing by 24% of total government spending on health in 2009. This estimate assumes good adherence to the set rules, particularly the respect of the referral system between the PHC centers and governmental hospitals, and the prescription of generic drugs. This might be ambitious to achieve in short term, nevertheless, the cost of the first stage of the project concerning the universal accessibility to essential services is perfectly affordable under current circumstances as shown in section VI.
- Primary Health Care: The MOPH-NGOs-Municipalities partnership
Primary Health Care services have proved to achieve significant outcomes compared with the modest resources they need. In addition, the contractual relationship of the MOPH with NGOs have contributed to streamlining PHC services provided by NGOs and to rationalizing the spending through shifting more funds towards promotion and prevention. This relationship is based, on one hand on the centers’ commitment to improve the health status of the community by providing a comprehensive package of PHC services according to WHO’s definition; And, on the other hand, the MOPH provision of free-of-charge vaccines and essential drugs in addition to setting quality standards and clinical protocols, as well as ensuring the required training of NGOs Staff. What distinguishes this relationship is the MOPH in-kind contributions (replacing the conventional fee-for-service reimbursement), against centers' commitment to achieve better health outcomes. This mechanism avoids incentives for over consumption and encourage tailoring interventions according to community’s needs. This relationship constituted a more effective alternative compared to traditional financial subsidies provided by other Ministries to NGOs, whereby the government has not been able to control spending or even evaluate the results of its investment. By their nature, the MOPH contributions, whether related to its normative role or to the supply of vaccines and generic drugs, cannot serve but the intended purpose of the contract. On the other hand, the involvement of Municipalities as third parties enhances community participation in orienting, managing, and evaluating PHC services.
Strengthening the network of primary health care centers, and linking them to government hospitals through a referral system, is a key pillar of the national health strategy. This network is covering gradually all cities, neighborhoods and villages, benefiting from a geographic information system indicating the groups of habitats that are to be included.
Achieving Universal Health Coverage in Lebanon requires the adoption of government financing modalities linked to community enrollment of citizens providing them foremost access to preventive services, early diagnosis and early treatment, which will reflect positively, not only on the health status and budget of households, but also on public health and total health expenditure.
Strengthening the network of primary health care centers, and linking them to government hospitals through a referral system, is a key pillar of the national health strategy. This network is covering gradually all cities, neighborhoods and villages, benefiting from a geographic information system indicating the groups of habitats that are to be included.
Achieving Universal Health Coverage in Lebanon requires the adoption of government financing modalities linked to community enrollment of citizens providing them foremost access to preventive services, early diagnosis and early treatment, which will reflect positively, not only on the health status and budget of households, but also on public health and total health expenditure.
- Community health coverage to ensure universal accessibility to a basic benefit package
This is a decentralized coverage design consisting of the following:
- An essential basket of preventive and curative services will be available to all the population with no exceptions, and are provided through the network of PHC centers and governmental hospitals. The program targets primarily individuals not covered for ambulatory care by other insurance schemes.
- A catchment area for each health center within the national PHC network is defined, and the health center is connected to a governmental hospital through a referral system.
- A steering committee will be created in each catchment area to establish a community based enrollment system with representatives of the local authorities. The committee initiates activities to create awareness and attract people, especially the poor and the marginalized.
- Each beneficiary should first join one of the health centers chosen in his/her geographic area which will be his/her first point of contact with the health system. The Center will refer applicants to the designated governmental hospital in the area to complete their medical check up.
- The health center provides preventive and primary health care services including clinical and diagnostic tests for early detection of chronic diseases. Whenever the needed tests or treatment are not available at the health center, the patient is referred to the outpatient department in the district governmental hospital for investigation, treatment or hospitalization if needed.
- Referrals from the district governmental hospital to more specialized governmental hospitals, or to the central governmental university hospital in Beirut will be done when needed.
- Whenever the case cannot be treated in governmental hospitals, the patient will then be covered by the MOPH for treatment in a private hospital provided he/she follows the proper referral channels.
- Enrollment in the network and issuance of the health card will be for free for the poorest who will also benefit from co-payment exemption for needed services. The poorest will be identified by the Ministry of Social Affairs (MOSA) Poverty Targeting project. The MOSA will cover their health card fees and co-payment.
- The individual’s enrollment fee is determined so that the family’s annual contribution does not exceed a certain lump sum. Enrollment of those not identified by the poverty project requires buying the health card over two installments: The first paid to the public hospital, the second to the health center. Children and adolescents in the family receive the card for free.
- As soon as the first installment is settled, the insured will benefit from a free consultation and medical screening tests as appropriate to his gender and age, and the infants will get completely immunized as per the national immunization calendar. The Governmental hospital will establish an electronic medical record for each enrolled which will be electronically sent to the referring health center and the MOPH at the same time.
- The health center provides the MOPH with a list of all the enrollees, and the MOPH issues a membership card and establishes a unified database for all beneficiaries linked to health centers and governmental hospitals.
- The relationship between the MOPH and the NGO running the health center is governed by a contractual agreement which include the municipality as partner. The steering committee will make sure that services are provided to beneficiaries according to the contract. From its part, the municipality would contribute to the upgrading of the center’s services according to community needs.
- The MOPH provides financial support for each center according to the number of enrollees, in addition to providing essential drugs and vaccines (imported through the UNICEF) and drugs for chronic illnesses (purchased through the YMCA), as well as providing necessary training and technical support.
- The MOPH contracts with government hospitals to provide outpatient services not available in the health center such as specialized consultations, laboratory tests and diagnostic services, and covers the necessary costs.
- Drug prescriptions and tests will be administered according to well defined protocols. The MOPH will provide only generic medicines while health centers and governmental hospitals would adhere exclusively to the essential drugs list.
- This scheme does not cover neither consultations in private clinics and laboratory tests in private labs, nor drugs purchased from private pharmacies.
- Private insurance companies and mutual funds are allowed to collect the second installment of the health card and issue in return a complementary health insurance policy to those who choose to do so.
- Financing Model and Financial Implications
This is not a project for establishing a “health insurance” financing model funded by adherents’ contributions. Pooling risks through mandatory adherence is not considered as a requirement for two reasons: first, bad risks that incur expensive tertiary care are already covered by the MOPH for hospitalization and second, the Government decision is to allocate treasury funding for this kind of essential health services. This would rather be a voluntary enrollment system to constitute a catchment population that is loyal to a particular health center. The enrollment fee serves two objectives: first, it makes the NGO liable to the enrollee who in return would claim his rights to get the whole range of services included in the package, and second, to transform into prepayment some of the OOP spent on health care when purchasing the services, while reducing it significantly.
On the other hand, the enrollment would allow for a kind of capitation based financing where the MOPH links its payment to the number of enrollees avoiding thus inflationary fee for service reimbursement. This system would also incite the health center to provide quality services in order to attract enrollees and therefore generate more revenues and at the same time promote early diagnosis and rational follow up.
This program is expected to double the revenues of the health centers in the first year, enabling them to attract additional qualified human resources and enhancing their capability to providing quality services.
The increase in the activities of the centers will lead to increased demand for essential medicines provided or funded by the MOPH and will incur additional administrative burdens on the primary health care department, which will require additional human and financial resources. The expected cost of this initial phase is 60 Billion LBP from which the government will have to contribute with 40 Billion LBP representing only around 6% of the 2013 MOPH budget.
[1] This working paper elaborated in April 2014 was behind the development of the WB project on UHC that started implementation mid 2016.
[2] Director General of the Ministry of Public Health.
Professor at the Faculty of Medicine- Lebanese University
On the other hand, the enrollment would allow for a kind of capitation based financing where the MOPH links its payment to the number of enrollees avoiding thus inflationary fee for service reimbursement. This system would also incite the health center to provide quality services in order to attract enrollees and therefore generate more revenues and at the same time promote early diagnosis and rational follow up.
This program is expected to double the revenues of the health centers in the first year, enabling them to attract additional qualified human resources and enhancing their capability to providing quality services.
The increase in the activities of the centers will lead to increased demand for essential medicines provided or funded by the MOPH and will incur additional administrative burdens on the primary health care department, which will require additional human and financial resources. The expected cost of this initial phase is 60 Billion LBP from which the government will have to contribute with 40 Billion LBP representing only around 6% of the 2013 MOPH budget.
[1] This working paper elaborated in April 2014 was behind the development of the WB project on UHC that started implementation mid 2016.
[2] Director General of the Ministry of Public Health.
Professor at the Faculty of Medicine- Lebanese University
Related video

Sitemap 
© Copyrights reserved to Ministry of Public Health 2026